Minimizing the risk of EHP spread is crucial:
White Feces Syndrome (WFS) is characterized by floating white fecal strings in shrimp ponds (Penaeus monodon and P. vannamei) in Southeast Asian countries. The syndrome has been found to be associated with several farm-level issues, including slow growth, significant size variation, reduced feed intake, and prolonged chronic mortality.
In countries where WFS has been studied, other enteric diseases affecting the shrimp hepatopancreas have also been demonstrated, including the microsporidian Enterocytozoon Hepatopenaei (EHP), acute hepatopancreatic necrosis disease caused by Vibrio parahaemolyticus (VpAHPND), and septic hepatopancreatic necrosis (SHPN) caused by Vibrio sp. Figure 1 shows Southeast Asian countries that have reported WFS and other enteric diseases.
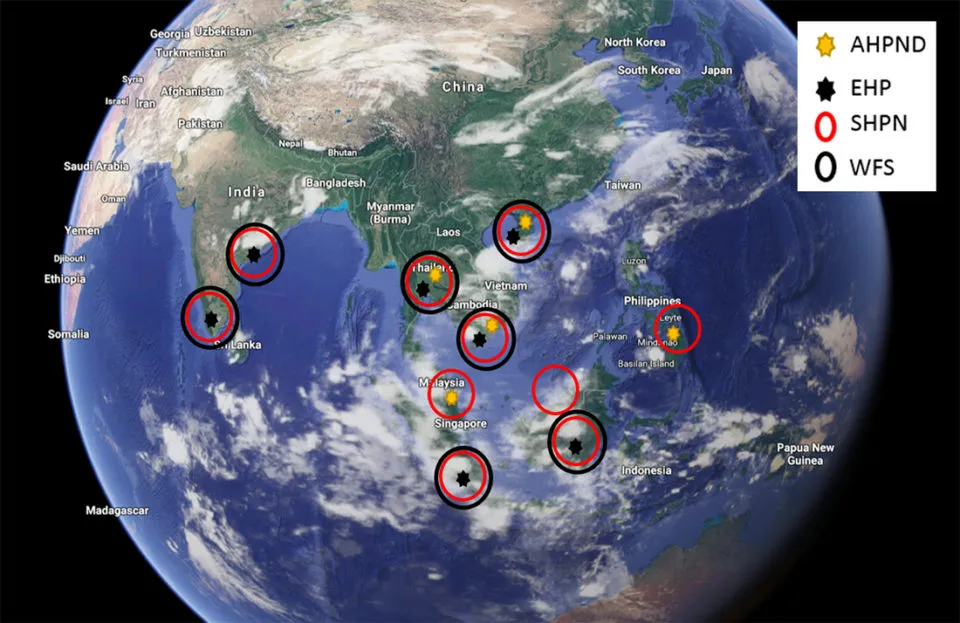
Figure 1. Enteric diseases including White Feces Syndrome (WFS), EHP, AHPND, and SHPN in Southeast Asian countries
EHP - an intracellular parasite replicating in the cytoplasm of tubule epithelial cells affecting the hepatopancreas, is a pathogen affecting farmed P. vannamei shrimp primarily in several Southeast Asian countries, including Indonesia, Vietnam, China, India, and Malaysia. The main clinical signs of EHP-infected shrimp are slow growth, leading to increasingly pronounced size variation. In later stages, EHP-infected shrimp often exhibit soft shells, lethargy, reduced feed intake, and empty guts. Histological analysis of infected tissues shows several developmental stages, including parasitic and spore stages.
Some previous articles have concluded the causes of WFS, including Vibriocholera, Gregarine, Bacilloplasma sp., and Phascolarctobacterium sp. Some studies also suggest that EHP is not the causative agent of WFS. Based on these differences related to WFS, we conducted a study to determine the potential relationships between WFS and enteric diseases such as EHP, in two different regions of the world where EHP had been previously reported.
The study was conducted in an Asian country with a history of EHP and WFS. Samples were collected from ponds, one group of shrimp showing WFS symptoms and another not showing symptoms. Hepatopancreas and fecal samples were collected and analyzed by histology and qPCR for EHP.

Figure 2. Shrimp samples exhibiting WFS (top left); observed white discoloration of the extruded gut (right); hepatopancreas exhibiting WFS showing severe deformation and melanization and absence of R cells (bottom left)
The results showed a clear difference in EHP copy numbers between the two groups. The average copy number in the WFS-infected group was 4 × 107 copies/ml DNA compared to 1 × 105 copies/ml DNA in ponds without WFS. This indicates that shrimp exhibiting WFS may have a higher EHP infection potential than shrimp without WFS. qPCR on fecal strings from the same shrimp showed similar results; that is, shrimp exhibiting WFS showed higher EHP copy numbers in fecal strings compared to shrimp not exhibiting WFS.
WFS in the Americas:
In the Western Hemisphere, in 2016, we reported the presence of EHP in farmed shrimp. EHP-infected shrimp exhibited clinical signs similar to those in Southeast Asian countries, such as reduced feed intake, slow growth, and size variation. Two years later, we described the first case of WFS in regions where we had previously reported the presence of EHP-infected whiteleg shrimp (Penaeus vannamei) cultured in Latin America. White fecal strings and shrimp exhibiting white feces along the digestive tract were similar to samples found in some Southeast Asian countries where WFS occurs.
Shrimp exhibiting WFS were analyzed by both H&E and PCR to identify the etiological agent associated with this disease manifestation. The results of PCR and H&E are shown in Figure 4.
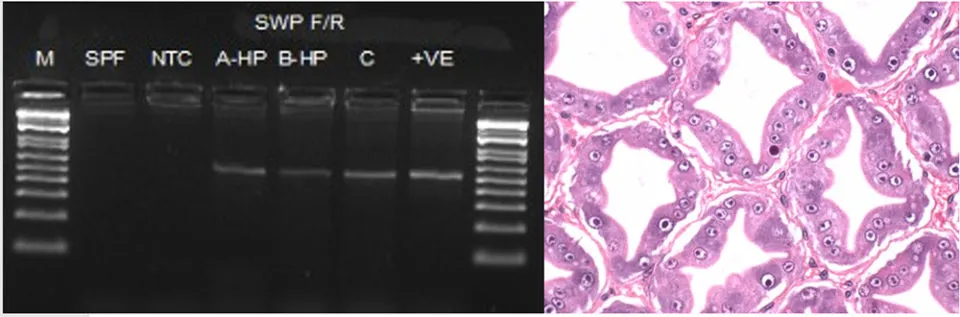
Figure 3. Detection of EHP in whiteleg shrimp (Penaeus vannamei) infected with WFS in Latin America. PCR was performed to amplify the spore wall protein (SWP) gene (left) and H&E of samples are shown in the right image (20X)
Correlation between SHPN and WFS:
In both Southeast Asia and Latin America where WFS has been studied, EHP is not the only pathogen associated with WFS. Shrimp analyzed by H&E showed that in addition to EHP, hepatopancreatic necrosis lesions were also associated with SHPN (Figure 4).
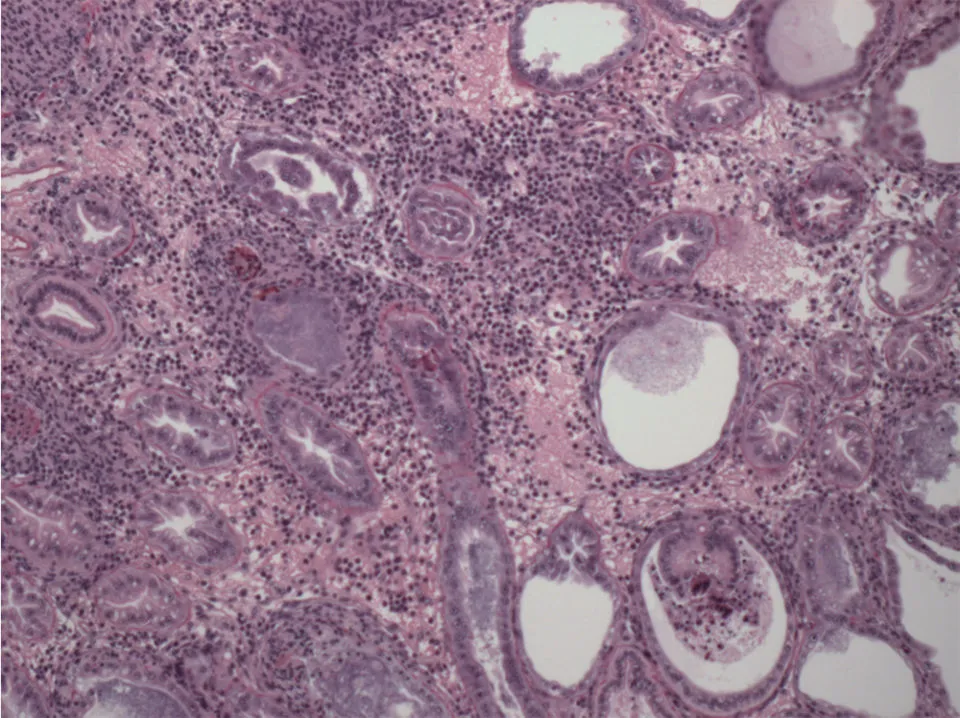
Figure 4. Examples of septic hepatopancreatic necrosis (SHPN) manifestations in P. vannamei (10X) from ponds with WFS
SHPN is a bacterial disease primarily caused by pathogenic or opportunistic Vibrio spp. Opportunistic Vibrio are always present in the hepatopancreas; however, when a primary enteric pathogen causes lesions in the hepatopancreas, these opportunistic Vibrio will affect the hepatopancreas and cause septic hepatopancreatic necrosis (SHPN).
According to Figure 5 and based on our analysis showing the relationship between WFS, EHP, and SHPN in ponds, WFS is a physiological response that can occur in shrimp affected by a combination of enteric diseases and potentially environmental factors.

Figure 5. The combination of primary enteric pathogens, opportunistic Vibrio spp., and environmental factors can cause WFS in EHP-infected regions
Conclusion:
From our study, a strong correlation can be observed between White Feces Syndrome (WFS) and EHP in regions with a history of EHP. EHP, in combination with other enteric pathogens (including SHPN) and environmental factors, can cause White Feces Syndrome.
In EHP-endemic regions, shrimp showing clinical signs of White Feces Syndrome indicate a rapid EHP infection process in ponds. White Feces Syndrome in the American shrimp industry could be a reflection of what happened in Southeast Asia 15 years ago, where EHP occurred sporadically but has now become one of the main risk factors for the shrimp industry in this region. Biosecurity strategies must be implemented to minimize the risk of EHP spread in the Americas.
Source: www.aquaculturealliance.org
Abridged translation by: Trần Thị Thúy Quyên






